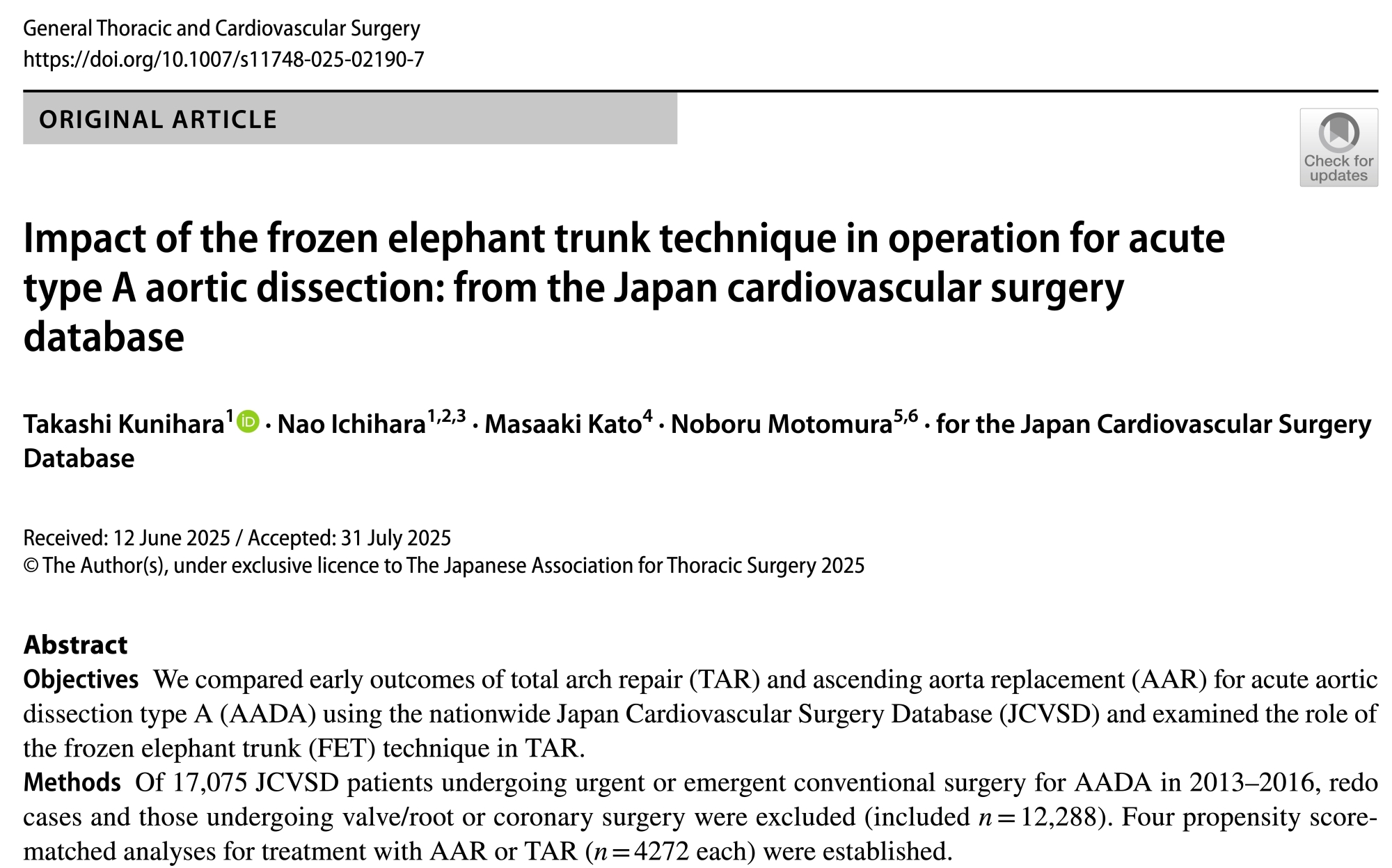
大動脈弁形成術の技術サポートを行いました
広島大学で大動脈弁形成術に関わる機会をいただきました。お役に立てて光栄です。

広島大学で大動脈弁形成術に関わる機会をいただきました。お役に立てて光栄です。
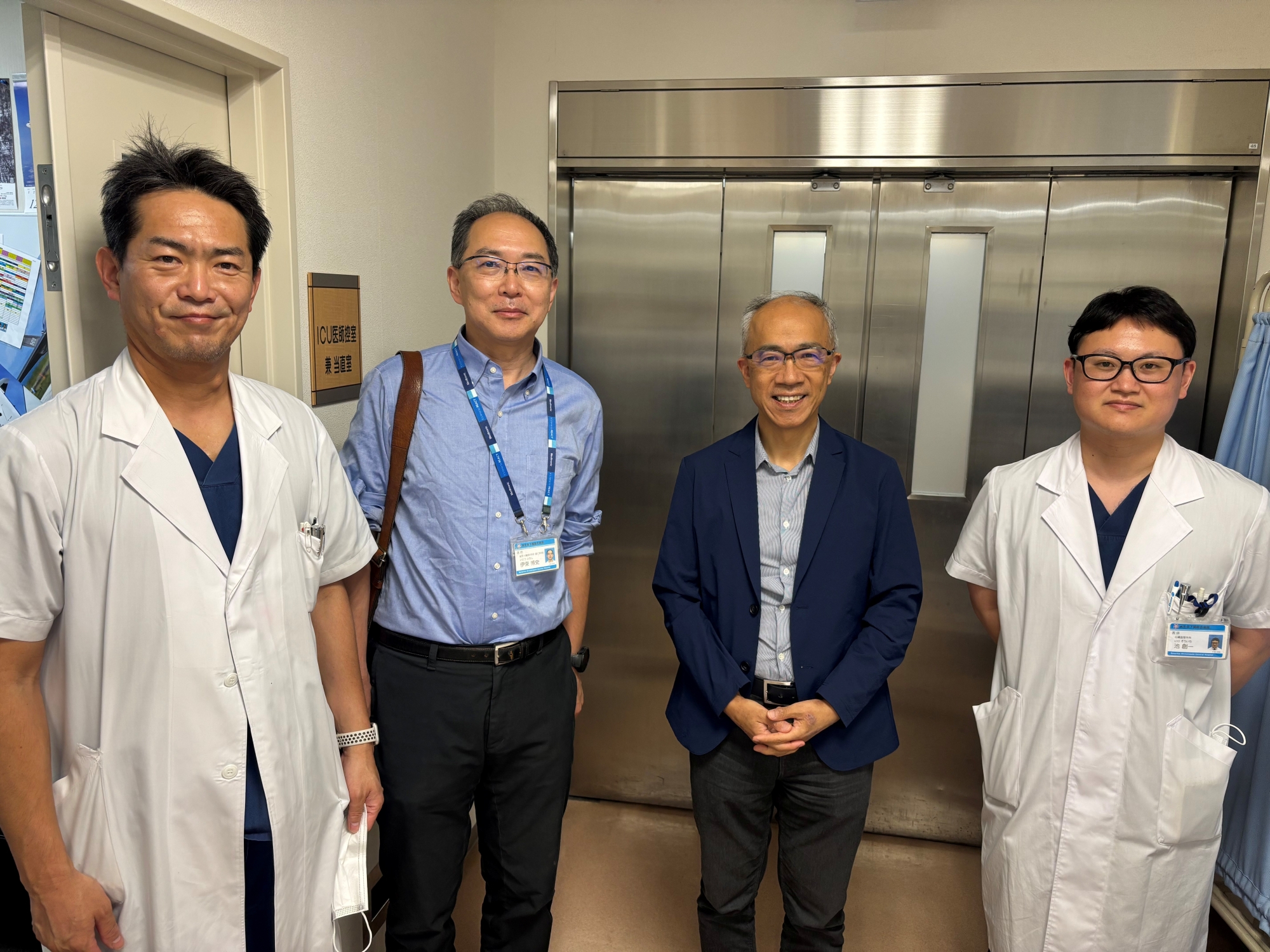
信州大学医学部附属病院において大動脈弁形成術の技術サポートを行いました。弁輪形成術の効果を外科医の皆さんにも実感してもらうことができ、この手術がさらに広まることを期待します。
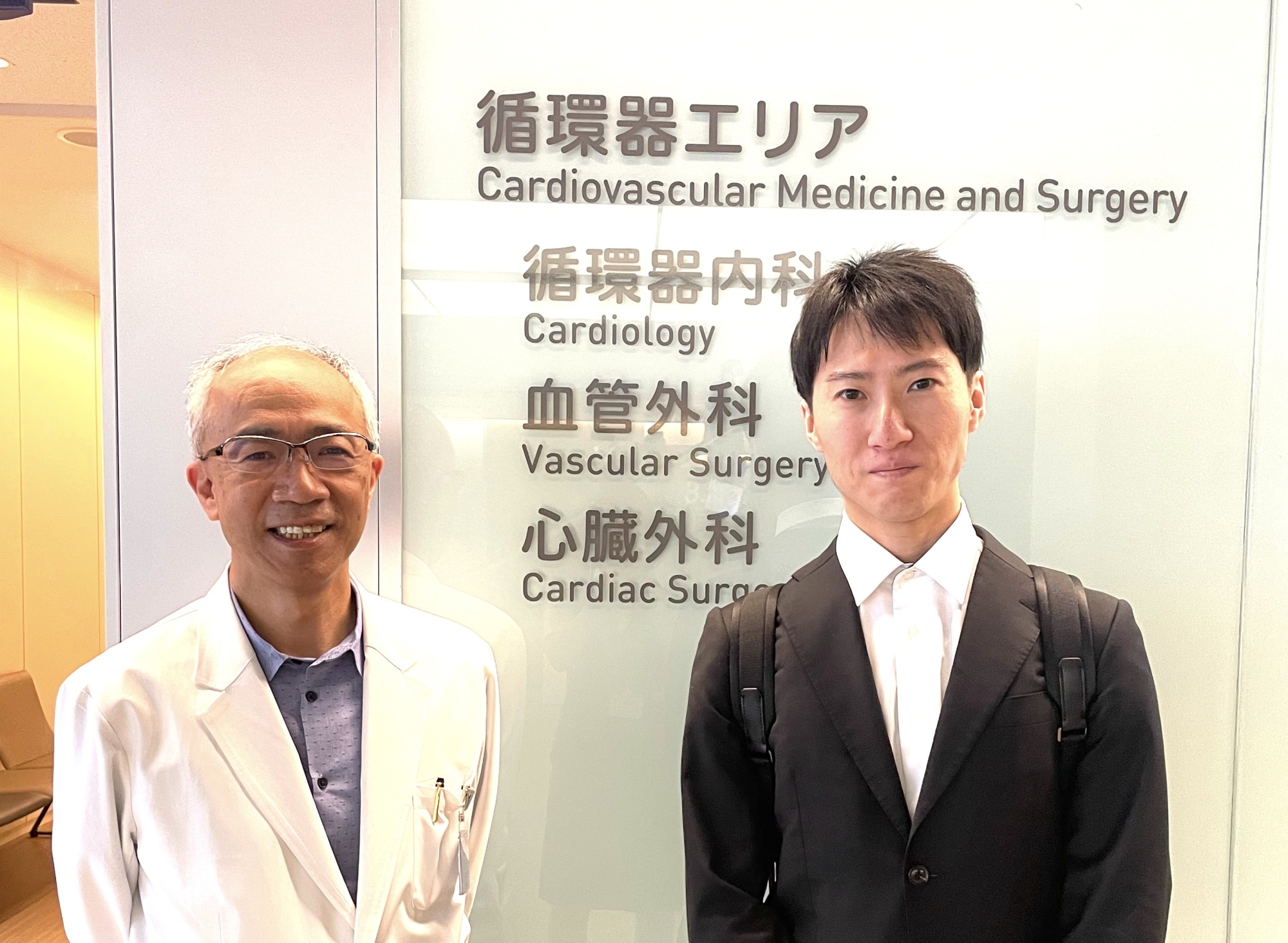
関西地方の病院で若年の大動脈弁閉鎖不全症患者さんに大動脈弁形成術を施行し、無事成功しました。人工弁を植え込むことを回避でき、患者さんに大変喜んでもらえました。
2026.5.28

関西地方の病院で大動脈弁形成術の技術支援を行い、無事うまく行きました。
2026.4.2

國原先生のインタビュー第1回が、3/11より配信スタートしました!
先生のこれまでの歩みや、大切にされている想いをじっくりお話しいただいています。
https://usci.koelab.net/
https://podcasts.apple.com/jp/podcast/id1599035676
▼Spotify
https://open.spotify.com/show/2u2Yk4DTXH9ctfHeoX1OOR
通勤時間やちょっとしたスキマ時間に、ぜひ聴いてみてください。
今後は毎週水曜日に新エピソードを更新していきます。
📅 3/25(水)第3回
📅 4/1(水) 第4回
これからの配信もお楽しみにしてください🎧
2026.3.17
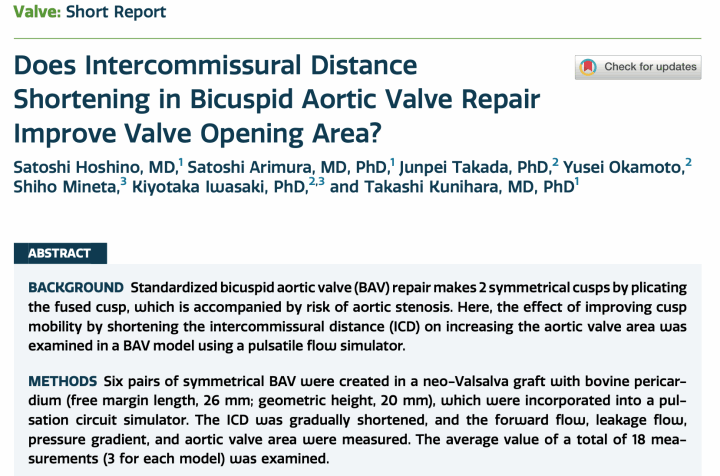
早稲田大学 先端生命医科学センター (TWIns)と共同で行なっている大動脈弁形成術に関する研究の成果を教室の星野医師が学位論文としてまとめてくれました。
ご興味のある方はご覧になっていただければ幸いです。
2026.3.6
第199回日本胸部外科学会関東甲信越地方会において教室の石割が急性大動脈解離症例におけるselective sinus replacement法について発表し、熱い議論が繰り広げられました。
2025.11.19

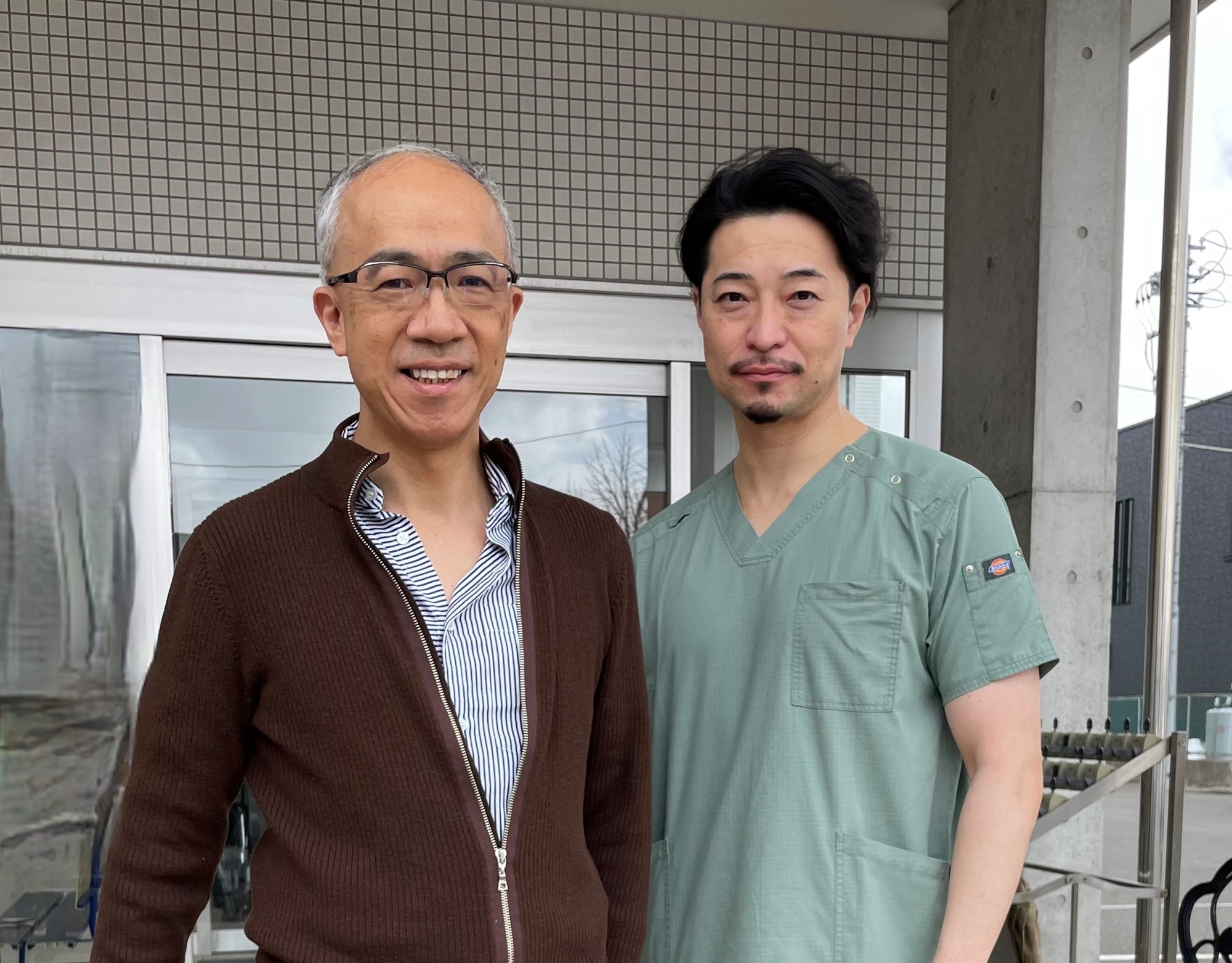
札幌の某病院において大動脈弁形成術を施行し、無事うまくいきました。
中央は華岡青洲直筆の書です。
2025.2.19




9月20日川越市ラ・ボア・ラクテにて開催された第8回圏央Heart Disease Forumで國原が講演を務めました。
特別講演II 19:45~20:30
「乳頭筋を活かした僧帽弁手術」
演者 國原 孝
座長 中嶋 博之 先生
埼玉医科大学国際医療センター 心臓血管外科 教授


7月23日千葉市において開催された第346回心電図を読む会 学術講演会において國原が特別講演を務めました。
「高齢者に対する心臓血管外科治療は恐くない?」
東京慈恵会医科大学 心臓外科 主任教授 國原 孝
座長:千葉ハートクリニック 院長 今牧 瑞浦 先生


7月12日13時〜16時 慈恵医大2号館901会議室でYacoub手術、PVR、Cone手術のwet labo、AVSD手術のdry laboを開催しました。
参加者:森田紀代造 宇野吉雅 中尾充貴 木南寛造
参加協力:エチコン



Friday 8th June 2018 (day 1)
Session 3 (13:00-14:30): Aortic Disease and Valve Repair Äb0
Moderators: Takashi Kunihara (Tokyo); Jeng Wei (Taipei); Artur Lichtenberg (Düsseldorf)
「Aortic root reconstruction and valve repair – from patient profile and therapy planning to optimal long-term results 」

In the era of aortic valvuloplasty (AVP), threshold for surgical intervention for aortic regurgitation (AR) can be classified into the following three stages:
1) Indication for aortic valve surgeryLeft ventricular end-diastolic/systolic diameter of 65/50mm and left ventricular ejection fraction of 50% is currently defined as threshold for intervention. However, in contrast to aortic valve replacement for cases with aortic stenosis, early surgical outcomes for AR are excellent. With improving long-term results of AVP, we hope earlier intervention will be recommended for low risk patients in the future when AVP is aimed. Early indication will also facilitate AVP.
2) Indication for AVP Currently, most etiologies of AR can be repaired, however, type III lesion is the most challenging case. Cusp height less than 16mm in tricuspid valve and less than 19mm in bicuspid valve is considered as contraindication for AVP. Of course they can be repaired by cusp-extension with a pericardial patch, although the long-term outcomes are still encouraging. Decision-making should be based on negotiation with each case.
3) Indication for root replacementCurrent guidelines recommend aortic root replacement in cases with root diameter more than 45mm when AVP is performed. However, root replacement has another role to facilitate AVP with respect to arrangement of commissural orientation in addition to the prevention of rupture or dissection. Especially in cases with bicuspid aortic valve, this threshold should be lowered. Considering the valve-related adverse events, AVP has an important role in surgical repair of AR.
We believe earlier indication may improve the quality of life of patients with AR necessitating surgical intervention.
「Lessens learned from Japanese registry of valve-preserving root replacement」
~日本のAortic valve academyのレジストリーの集計結果を発表~
2017/3/26
金沢で開催された第81回日本循環器学会で國原が当院での研究成果を発表しました。
「Impact of Aortic Valvuloplasty for Aortic Regurgitation with regard to LV Reverse Remodeling and Transvalvular Hemodynamics」









































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}